
Leaky Gut: What the Science Actually Says (And What It Doesn’t)
- What “Leaky Gut” Actually Means
- The Science-vs-Hype Divide Around Leaky Gut
- Conditions Linked to Intestinal Permeability
- What Actually Causes Increased Permeability
- How People Actually Test for It (And Why Most Don’t Need To)
- The Supplement Industry’s Favorite Topic
- The Boring Stuff That Actually Works
- Diets Marketed for Leaky Gut — An Honest Take
- When to See a Doctor
- A 30-Day Gut Lining Support Plan
Last updated: April 24, 2026
Quick Answer: “Leaky gut” is the popular name for increased intestinal permeability — a real, measurable physiological state where the 4-week science-backed gut reset plan that supports the gut lining becomes more permeable than it should be. However, “leaky gut syndrome” as a standalone medical diagnosis is not currently recognized by mainstream medicine. Research does link altered intestinal permeability to conditions like celiac disease, Crohn’s, and IBS, but whether it causes those conditions or results from them is still actively debated. What genuinely helps is mostly unglamorous: whole foods, soluble vs insoluble fiber and daily targets, sleep, and how the gut-brain axis turns chronic stress into gut dysfunction management. Most supplements marketed for it are ahead of the evidence.
Somewhere between “leaky gut causes everything” and “leaky gut doesn’t exist” is where the actual science lives. If you’ve spent any time reading health content online, you’ve seen both extremes. Wellness influencers blame leaky gut for fatigue, brain fog, skin problems, depression, and autoimmune disease. Meanwhile, some conventional doctors wave it off entirely. Neither position is quite right. The underlying biology — increased intestinal permeability — is real, measurable, and genuinely interesting to researchers. The problem is that the term “leaky gut” has been borrowed by the supplement industry and stretched far beyond what the evidence supports. Let’s keep this practical: here’s what the research actually shows, where the honest uncertainty sits, and what’s worth doing about it — without a $90 supplement bundle.
Key Takeaways
- Increased intestinal permeability is real and can be measured in research settings, but “leaky gut syndrome” is not a recognized clinical diagnosis [1][2]
- The gut lining is a single-cell-thick barrier controlled by proteins called tight junctions — when these loosen, more particles cross through than normal
- Celiac disease, Crohn’s, and ulcerative colitis have the strongest evidence linking them to altered intestinal permeability [1]
- Stress, alcohol, NSAIDs, poor diet, and sleep deprivation are among the best-documented contributors to increased permeability [1][5]
- Gluten’s role is contested — the evidence does not conclusively link gluten to leaky gut in people without celiac disease [2]
- Zonulin is the only known reversible regulator of intestinal tight junctions and is an active area of pharmaceutical research [4]
- Most supplements marketed for leaky gut lack strong clinical evidence; a few (zinc carnosine, specific probiotic strains) show modest promise
- The lifestyle interventions with the most support are high-fiber diets, fermented foods, adequate sleep, and stress reduction
- Home test kits for leaky gut are largely unreliable and rarely change clinical management
- See a doctor if you have blood in stool, unexplained weight loss, persistent pain, or symptoms that don’t respond to lifestyle changes in 2–3 months
What “Leaky Gut” Actually Means
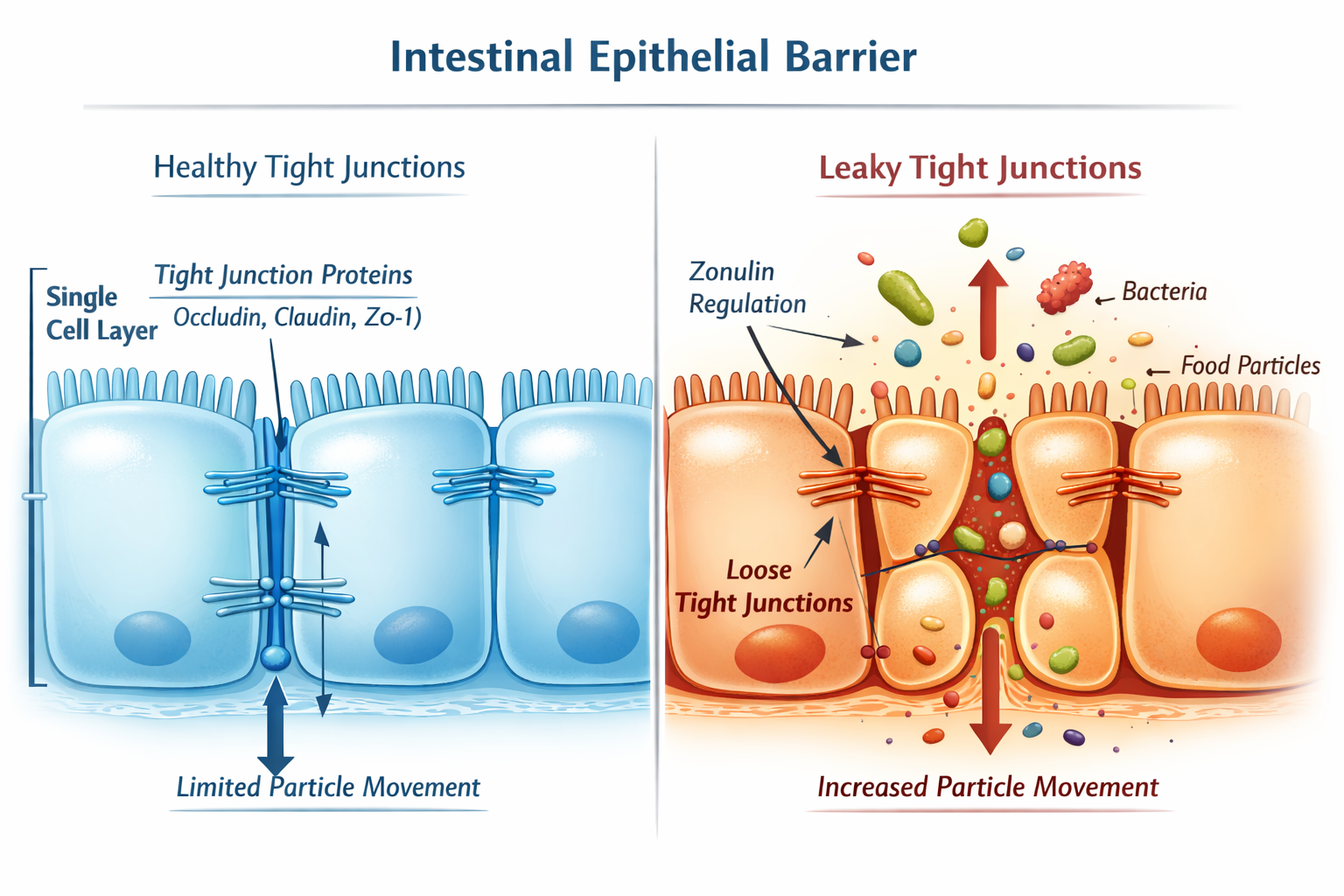
The simplest way to look at it is this: your gut lining is a single layer of epithelial cells — roughly one cell thick — that acts as a controlled barrier between the contents of your intestine and your bloodstream. Nutrients and water pass through in a regulated way. Most bacteria, toxins, and undigested food particles are supposed to stay out.
The cells in this lining are held together by structures called tight junctions — protein complexes that act like seals between adjacent cells. When those junctions work properly, the barrier is selective. When they loosen or become dysregulated, more material crosses through than it should. That’s increased intestinal permeability. That’s what people mean when they say “leaky gut.” [1][2]
A few things worth understanding clearly:
- It’s not a hole. The barrier doesn’t rupture. It’s a regulation issue — the gates become less selective, not broken.
- Some degree of permeability is normal. The gut is never a perfect seal. The question is whether permeability has shifted beyond the normal functional range.
- Zonulin is the only protein currently identified as a reversible regulator of tight junction function. It can be upregulated by environmental and dietary triggers, and it’s the basis of some of the most credible research in this area [4].
- The lactulose/mannitol test — measuring how much of two differently-sized sugar molecules appear in urine after oral ingestion — is the research standard for assessing permeability. It’s not widely used in clinical practice [2].
The name “leaky gut” is part of the problem. It sounds dramatic, implies something is broken, and makes it easy to market solutions. In plain English, it’s a shift in how well a cellular barrier regulates what passes through it. That’s a more accurate frame.
The Science-vs-Hype Divide Around Leaky Gut
Here’s the real issue: mainstream medicine and alternative health are talking about two different things, and neither side is being fully honest about it.
What mainstream medicine accepts:
- Increased intestinal permeability is a real, measurable physiological state [2]
- It is associated with several established medical conditions (more on those below)
- Certain factors — alcohol, NSAIDs, infection, chronic stress — can alter gut barrier function [1][5]
What mainstream medicine does not accept:
- “Leaky gut syndrome” as a standalone diagnosis with its own diagnostic criteria [1]
- The claim that increased permeability is the root cause of a wide range of non-GI conditions
- Most of the supplement-based treatment protocols marketed online
Where researchers are actively working:
- The role of zonulin as a therapeutic target (larazotide, a zonulin antagonist, has been evaluated in celiac disease clinical trials) [2]
- Microbiome-permeability interactions and how gut bacteria influence tight junction integrity [6]
- Whether permeability changes precede disease or follow from it — a genuinely unresolved question
“We’re in the middle of this science, not the end.” That’s not a reason to dismiss it. It’s a reason to be careful about claims made on either side.
The alternative health world jumped ahead of the evidence, attached leaky gut to nearly every chronic symptom, and built a supplement industry around it. That backfires because when the evidence doesn’t support the claims, the whole concept gets dismissed — including the parts that are legitimate. We need to separate fact from hype, not because the biology isn’t interesting, but because exaggeration makes it harder for people to make good decisions.
Conditions Linked to Intestinal Permeability
The evidence is not uniform across conditions. Some associations are well-established. Others are emerging. Some are being oversold. Here’s an honest breakdown. [1][2]
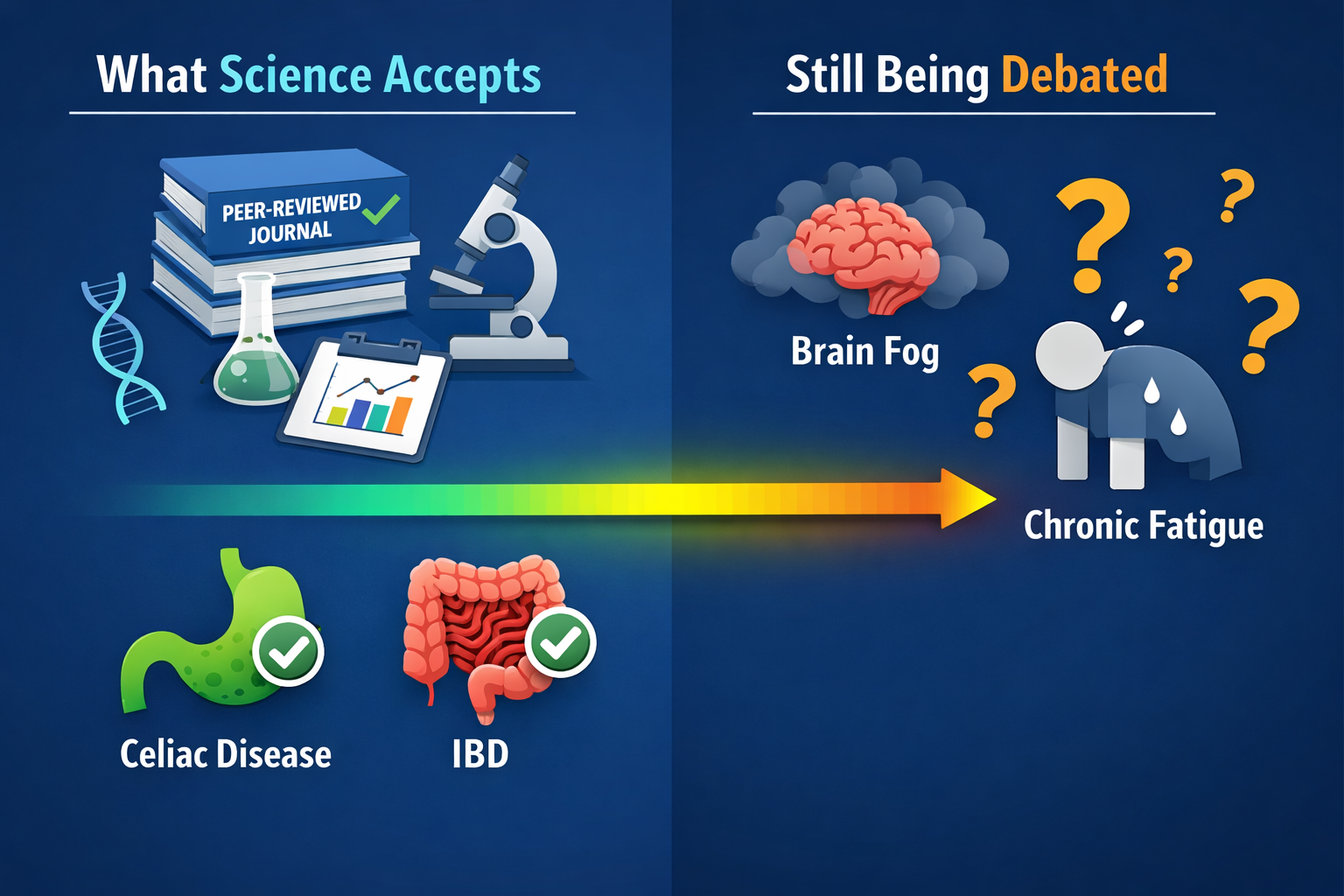
✅ Proven / Well-Established Association
- Celiac disease — altered intestinal permeability is a documented feature, and zonulin upregulation in response to gliadin (a gluten protein) is a key mechanism [2][4]
- Crohn’s disease — increased permeability is observed and may precede flares
- Ulcerative colitis — barrier dysfunction is a recognized component of disease pathology [1]
🔶 Strong Association / Plausible Mechanism
- Irritable bowel syndrome (IBS) — a subset of IBS patients show increased permeability, particularly post-infectious IBS [1]
- Type 1 diabetes — research suggests altered gut barrier function may play a role in autoimmune activation [1]
- Multiple sclerosis — gut microbiome and permeability research is an active area, with early findings suggesting a connection [7]
- Systemic lupus erythematosus — some studies show elevated permeability markers, though causality is unclear [1]
🔍 Debated / Early-Stage Research
- Depression and anxiety — the gut-brain axis is real, and some research links permeability to neuroinflammation, but the clinical picture is far from settled
- Brain fog and chronic fatigue — frequently cited online, limited direct evidence
- Certain skin conditions (eczema, psoriasis) — some association with gut how probiotics and prebiotics rebalance gut dysbiosis, permeability link is indirect
⚠️ Oversold Online
- Virtually every chronic symptom that doesn’t have a clear diagnosis has been attributed to leaky gut somewhere on the internet. That doesn’t mean the connection exists. The evidence for most of these claims is either absent or very preliminary. I would be careful with that.
What Actually Causes Increased Permeability
Several factors have reasonable evidence behind them. The list isn’t exotic. Most of it points back to the same lifestyle variables that affect nearly every aspect of health.
| Factor | Evidence Level | Notes |
|---|---|---|
| Chronic stress | Moderate | Stress-induced permeability increases observed in studies; causal role not fully established [2] |
| Heavy alcohol use | Strong | Causes epithelial cell death and damages tight junction proteins; occasional drinking likely minimal risk [1] |
| NSAIDs (long-term) | Strong | Ibuprofen, naproxen — documented contributors to increased permeability [5] |
| Ultra-processed food / low fiber diet | Moderate | Emulsifiers in processed foods show effects in lab studies; direct human evidence still limited [1] |
| Gut infections | Moderate | Giardia, C. difficile history linked to post-infectious permeability changes |
| Chronic sleep deprivation | Moderate | Sleep disruption affects gut barrier function through inflammatory pathways |
| Gut dysbiosis | Moderate | Imbalanced gut microbiome is associated with altered tight junction regulation [6] |
| Certain medications | Moderate | Chemotherapy agents, some antibiotics — recognized contributors |
A few things worth noting:
- Gluten is frequently highlighted in lay literature, but the evidence linking it specifically to leaky gut in people without celiac disease is not conclusive [2]. Cutting gluten is not a universal fix.
- Changes in permeability are not always harmful. The gut lining is dynamic. Temporary increases in permeability don’t automatically lead to disease — context matters, and the relationship between permeability changes and symptoms is still being worked out [2].
How People Actually Test for It (And Why Most Don’t Need To)
In plain English: reliable testing exists in research settings, but it’s rarely available or necessary in clinical practice.
The main methods:
- Lactulose/mannitol ratio test — the research gold standard. You drink a solution containing two sugar molecules of different sizes, then measure how much of each appears in urine. A higher ratio suggests increased permeability. Used in research, not standard clinical care [2].
- Zonulin blood test — increasingly available through functional medicine practitioners. Measures circulating zonulin as a proxy for permeability. Useful as a general indicator, but not definitive on its own [4].
- Intestinal tissue biopsy, confocal laser endomicroscopy, endoscopic mucosal impedance — accurate but invasive, reserved for specific clinical investigations [2].
- At-home “leaky gut” test kits — most measure markers that are not well-validated for this purpose. The evidence base for interpreting these results in a clinically meaningful way is thin. I wouldn’t spend money on them.
From a practical point of view: if you have GI symptoms, fatigue, or other concerns, the more useful path is addressing the lifestyle factors that are known to affect gut barrier function — and seeing a doctor if symptoms are significant. Testing for permeability without that foundation rarely changes what you should do next.
The Supplement Industry’s Favorite Topic
This is where hype gets in the way. The leaky gut concept has generated a large supplement market, and the evidence behind most of those products doesn’t match the marketing. Here’s an honest breakdown.
L-Glutamine
An amino acid used as fuel by intestinal epithelial cells. Some evidence suggests it may support gut barrier function, particularly in clinical settings like post-surgical recovery or chemotherapy. Evidence in otherwise healthy people with mild permeability changes is mixed. It’s generally safe, and it might help some people — but the effect size in healthy adults is likely modest.
Collagen / Bone Broth
Popular and not harmful. The direct evidence that collagen supplementation repairs intestinal tight junctions in humans is weak. Bone broth contains some amino acids relevant to gut tissue, but the concentrations are low and the clinical data isn’t there yet. Worth including in a varied diet; not worth paying a premium for as a “gut repair” product.
Zinc (especially zinc carnosine)
This is probably the most evidence-supported supplement in this space. Zinc carnosine has shown some ability to support gut lining integrity in small studies. Zinc deficiency itself impairs gut barrier function, so if you’re deficient, correcting that matters [5]. Not a magic fix, but a reasonable consideration.
Probiotics
The evidence here depends entirely on the strain. Some specific strains — Lactobacillus rhamnosus GG, Bifidobacterium longum — have reasonable evidence for gut barrier support in specific contexts. “Probiotic” as a generic category tells you almost nothing. If you’re going to try one, look for a product with a specific, studied strain and a clear indication [6].
“Gut Repair Formulas” with 15 ingredients
Marketing first, science second. Combining multiple ingredients with limited individual evidence doesn’t multiply the effect. It usually just multiplies the cost.
The main takeaway is this: a few targeted supplements have modest supporting evidence. Most don’t. None of them substitute for the lifestyle factors that have the strongest evidence base.
The Boring Stuff That Actually Works
The evidence suggests that the most effective interventions for gut barrier support are the least exciting ones. This is where most online articles fail — they skip past the basics to sell you something. I prefer to look at what actually works.

High-fiber diet
Fiber maintains the intestinal mucous membrane, feeds beneficial bacteria that produce short-chain fatty acids (SCFAs), and may enhance tight junction protein expression. No studies have formally evaluated fiber as a leaky gut “treatment,” but the mechanistic and epidemiological evidence is strong [2]. Aim for 25–35g per day from whole food sources.
Fermented foods
Sauerkraut, kimchi, kefir, plain yogurt, and kombucha introduce beneficial bacteria and may support microbiome diversity. A 2021 Stanford study (not in our source list, so I won’t cite it directly) drew attention to fermented foods and microbiome diversity — the general principle is supported across multiple lines of evidence [6].
polyphenols and anti-inflammatory foods that support gut lining health
Berries, olive oil, green tea, dark chocolate, and colorful vegetables contain polyphenols that have anti-inflammatory effects and may support gut barrier integrity. The mechanisms are plausible; the direct human evidence for permeability specifically is still developing.
Stress management
Chronic stress is a documented contributor to permeability changes [2]. Practical stress reduction — whether through exercise, sleep, social connection, or structured relaxation — matters here. There’s no magic in it, but it’s not optional either.
Sleep (7+ hours)
Sleep deprivation increases systemic inflammation and impairs gut barrier function. Getting consistent, adequate sleep is one of the highest-return interventions for overall complete gut health and digestive wellness guide. Start with what gives the biggest return.
Moderate exercise
Regular moderate exercise is associated with improved gut microbiome diversity and reduced intestinal inflammation. Excessive high-intensity training without adequate recovery may temporarily increase permeability — context matters.
Reducing chronic NSAID use
If you’re regularly taking ibuprofen or naproxen for pain management, that’s worth discussing with your doctor. The gut barrier impact of long-term NSAID use is well-documented [5]. Alternatives may be worth exploring.
The basics still do the heavy lifting. Keep it simple and consistent.
Diets Marketed for Leaky Gut — An Honest Take
Several specific diets are promoted as solutions for leaky gut. Here’s what the evidence actually supports.
GAPS Diet (Gut and Psychology Syndrome)
Highly restrictive, eliminates grains, processed foods, and most sugars. The theoretical framework is interesting; the clinical evidence is weak. It’s hard to sustain and lacks the research base to justify its restrictions for most people.
Autoimmune Protocol (AIP)
An elimination diet that removes grains, legumes, dairy, eggs, nightshades, nuts, and seeds, then reintroduces them systematically. It’s useful as a diagnostic tool to identify personal food triggers — particularly for autoimmune conditions. It’s not a permanent diet and shouldn’t be treated as one.
Low-FODMAP Diet
Well-supported for IBS symptom management. It works by reducing fermentable carbohydrates that can cause gas and the real causes of bloating and how to match the fix. It’s not specifically a “leaky gut” intervention, and it’s intended as a short-term diagnostic and management tool, not a long-term eating pattern.
Whole-foods diet
The least exciting option and the one with the most consistent evidence. Minimally processed foods, plenty of plants, adequate fiber, fermented foods included. It doesn’t have a catchy name or a book deal, but it’s what the evidence points to most consistently.
When to See a Doctor
Lifestyle changes are a reasonable starting point for mild, non-specific GI symptoms. But some symptoms require medical evaluation. Don’t delay if you notice:
- 🔴 Blood in stool (red or black/tarry)
- 🔴 Unexplained weight loss
- 🔴 Severe or persistent abdominal pain
- 🔴 Night sweats or unexplained fever
- 🔴 Family history of IBD, celiac disease, or colorectal cancer
- 🟡 Symptoms that don’t improve after 2–3 months of consistent lifestyle changes
- 🟡 Significant fatigue, joint pain, or skin symptoms alongside GI issues
These symptoms need proper investigation — not a supplement protocol. A sensible starting point is always ruling out serious pathology before assuming lifestyle is the whole answer.
A 30-Day Gut Lining Support Plan
This is practical, free, and based on the interventions with the strongest evidence. No supplements required.
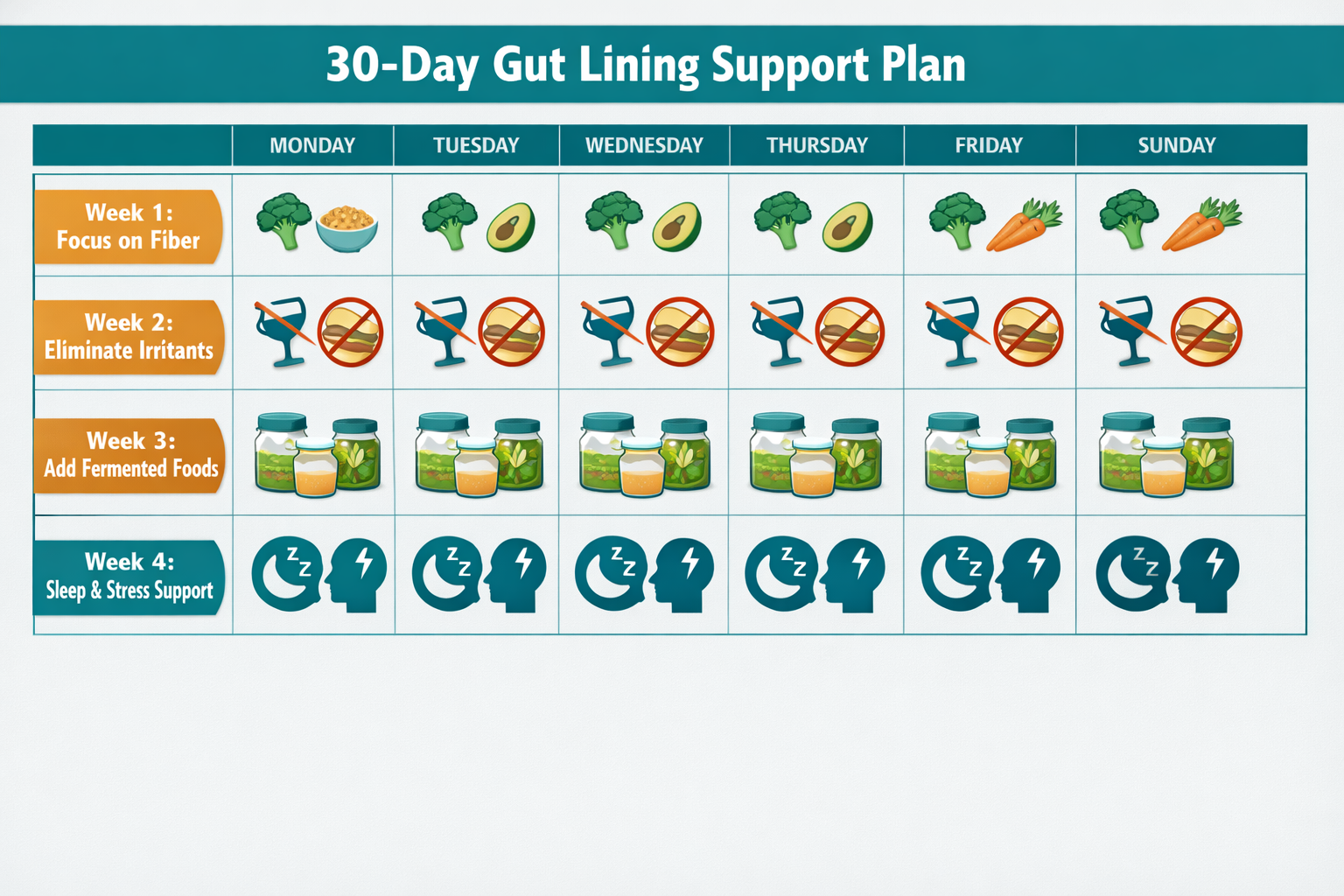
Week 1 — Add Fiber
- Target 25–35g of fiber per day from whole food sources
- Add one serving of legumes (lentils, chickpeas, black beans) per day
- Include at least 5 servings of vegetables and 2 servings of fruit
- Increase gradually to avoid bloating
Week 2 — Remove the Three Biggest Irritants
- Reduce alcohol — aim for at least 5 alcohol-free days this week
- Cut ultra-processed foods — anything with a long ingredient list of additives, emulsifiers, and artificial flavors
- Reduce NSAID use if you’re taking them regularly — speak to your doctor about alternatives
Week 3 — Add Fermented Foods
- Introduce one serving of fermented food per day: plain yogurt, kefir, sauerkraut, kimchi, or kombucha
- Start small (2–3 tablespoons) if you’re not used to fermented foods
- Add polyphenol-rich foods: berries, olive oil, green tea, dark chocolate (70%+)
Week 4 — Focus on Sleep, Stress, and Consistency
- Prioritize 7–8 hours of sleep per night
- Identify your main chronic stressor and address it directly — even one concrete step matters
- Review weeks 1–3 and consolidate what’s working
- Keep it simple and consistent going forward
Frequently Asked Questions
Is leaky gut syndrome a real diagnosis?
Increased intestinal permeability is a real, measurable physiological state. “Leaky gut syndrome” as a standalone medical diagnosis is not currently recognized by mainstream medicine — it lacks agreed diagnostic criteria and a defined clinical presentation. The biology is real; the syndrome label is not yet validated [1][2].
How long does it take to heal the gut lining?
There’s no established clinical timeline because “leaky gut” isn’t a formally diagnosed condition with defined healing endpoints. In conditions like celiac disease, gut lining recovery on a strict gluten-free diet can take months to years. For lifestyle-related permeability changes, consistent improvements to diet, sleep, and stress management over 4–12 weeks are a reasonable starting point — but individual variation is significant.
Do I need to cut out gluten?
Only if you have celiac disease or a confirmed non-celiac gluten sensitivity. The evidence linking gluten to leaky gut in people without celiac disease is not conclusive [2]. Eliminating gluten without a reason may reduce dietary variety and fiber intake — which could be counterproductive.
Can stress really cause leaky gut?
Some studies show stress-induced increases in intestinal permeability, and the gut-brain axis is well-established. However, the causal role of stress in developing a clinically significant permeability problem is not fully established — partly because it’s hard to isolate stress from other lifestyle factors [2]. Managing chronic stress is still worth doing, for this and many other reasons.
Are home test kits for leaky gut worth it?
Generally, no. Most home kits measure markers that are not well-validated for assessing intestinal permeability in a clinically meaningful way. The results rarely change what you should do, which is address the known lifestyle contributors regardless of test results. Save the money.
Is bone broth actually helpful?
It’s not harmful, and it can be part of a varied whole-foods diet. But the direct evidence that bone broth repairs gut tight junctions in humans is weak. It contains some relevant amino acids (glycine, proline) in modest amounts. Think of it as a useful food, not a therapeutic intervention.
What is zonulin and why does it matter?
Zonulin is a protein that regulates the opening and closing of tight junctions between intestinal epithelial cells. It’s the only known reversible regulator of intestinal permeability and is an active research target. Elevated zonulin is associated with increased permeability in conditions like celiac disease [4]. A drug called larazotide, which blocks zonulin’s effects, has been evaluated in clinical trials for celiac disease [2].
Can probiotics fix leaky gut?
Some specific probiotic strains have evidence for supporting gut barrier function in particular contexts. “Probiotics” as a generic category is too broad to make a meaningful claim. Strain specificity matters enormously. The evidence is promising but not definitive for most general-population use cases [6].
Conclusion
The leaky gut debate has been poorly served by both sides. Dismissing increased intestinal permeability as a myth ignores real biology and active research. Claiming it explains every chronic symptom and selling supplement bundles to fix it ignores the absence of evidence for most of those claims.
What we actually know: the gut barrier is a dynamic, regulated structure. It can become more permeable under certain conditions. That altered permeability is associated with several established medical conditions, and it’s an active area of legitimate research. What we don’t know: whether permeability changes cause most of the conditions it’s linked to, or result from them — and whether treating permeability directly changes clinical outcomes in most people.
What’s worth doing right now:
- Eat more fiber and whole plants
- Reduce alcohol, ultra-processed food, and chronic NSAID use
- Prioritize sleep and address chronic stress
- Add fermented foods to your regular diet
- See a doctor if you have significant or persistent symptoms
That’s not a supplement protocol. It’s not a 30-day detox. It’s the same evidence-based foundation that supports nearly every aspect of long-term health. There is no magic in it — but it’s what the evidence actually supports, and that matters more than what sounds impressive.
Truth over hype. Evidence first. That’s the only standard worth applying here.
References
[1] Leaky Gut – https://oshihealth.com/leaky-gut/ [2] Pmc11345991 – https://pmc.ncbi.nlm.nih.gov/articles/PMC11345991/ [3] What Is Leaky Gut – https://zoe.com/learn/what-is-leaky-gut[4] A Functional Medicine Protocol For Leaky Gut Syndrome – https://www.rupahealth.com/post/a-functional-medicine-protocol-for-leaky-gut-syndrome
[5] Leaky Gut Syndrome – https://www.goodrx.com/well-being/gut-health/leaky-gut-syndrome
[6] Leaky Gut Intestinal Permeability Science Guide – https://seed.com/cultured/leaky-gut-intestinal-permeability-science-guide/
[7] Video Gut Health In Multiple Sclerosis Actrims 2026 Expert Insights – https://www.neurologyadvisor.com/reports/video-gut-health-in-multiple-sclerosis-actrims-2026-expert-insights/

Dave James has spent 30+ years reading health and longevity research, and has run All Perfect Health for the past five. His background is in Australian mining and industrial engineering — disciplines built on questioning claims, measuring outcomes, and respecting evidence. He writes about what the research actually says, including where the experts disagree.
More about Dave & this site →