
Bloating: What Causes It and How to Actually Fix It
Last updated: April 21, 2026
- Featured Video: What Bloating Actually Is
- What Bloating Actually Is
- The 7 Real Causes of Bloating
- Which Type of Bloater Are You?
- What Actually Works: Fixes Matched to Type
- The Fiber Paradox
- Things That Usually Don’t Work (But Get Recommended Anyway)
- When Bloating Is Actually a Red Flag
- A 7-Day Bloating Reset
- The Gut-Brain Piece Most Articles Ignore
Quick Answer: Bloating is not one problem — it is several, each with a different cause and a different fix. The reason most advice fails is that it treats all bloating the same way. If you can identify which type of bloating you have, you can match it to the right solution and actually get results.
If you’ve ever buttoned your jeans at 8 AM and needed to undo them by 3 PM, you’re not alone — and you’re not broken. Bloating is one of the most common complete gut health and digestive wellness guides in every country health data covers, and research suggests that up to 96% of people with irritable bowel syndrome experience it as a primary symptom [2]. The problem isn’t that bloating is rare. The problem is that most advice about it is wrong for most people.
The standard recommendations — cut out gluten, drink lemon water, take a probiotics and prebiotics guide — are not useless. But they are generic. And generic advice applied to a specific problem rarely works. If you’ve tried the obvious fixes and you’re still looking for how to fix bloating that actually persists, there’s a good chance you haven’t yet identified the real cause.
This article gives you a way to work out which kind of bloating you have, then the fixes matched to that type. No hype, no detox plans, no products to buy. Let’s do this honestly.
What Bloating Actually Is
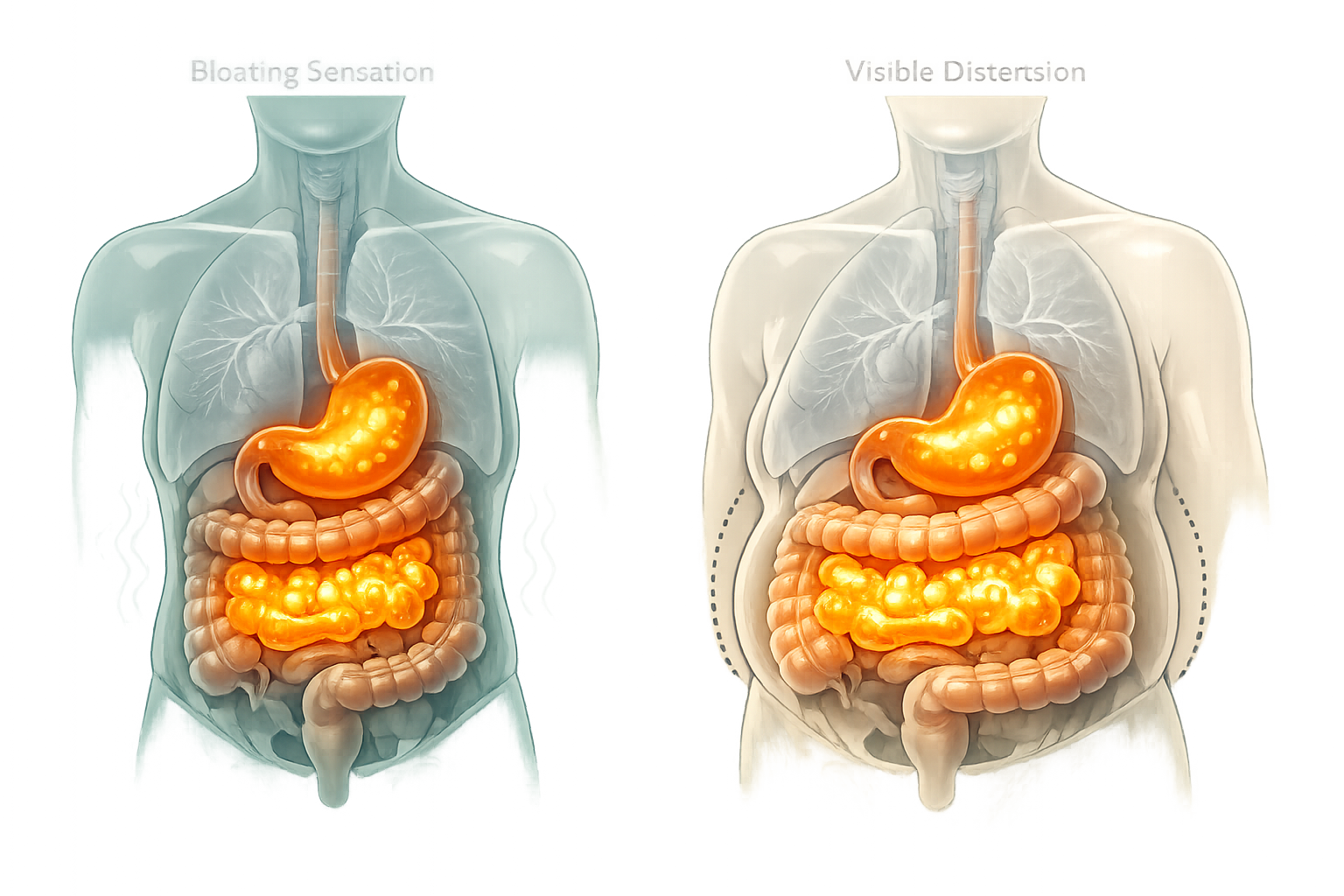
Bloating is a subjective feeling of fullness, tightness, or pressure in the abdomen. Distension is something different — it is a measurable, objective increase in abdominal circumference. These two things are related, but they don’t always occur together, and that distinction matters more than most articles acknowledge.
Expert insight: Dr. Alex Tatem. Dr. Alex Tatem is a peptide and regenerative medicine expert who has appeared on The Diary of a CEO. He specialises in root-cause approaches to metabolic dysfunction and gut health.
Research published in the American Journal of Gastroenterology found that bloating and distension frequently occur independently of each other [6]. Some people feel severely bloated with no visible change in abdominal size. Others show clear physical distension without reporting much discomfort. This tells us that the sensation of bloating is partly a neurological event — how the gut’s nervous system interprets pressure — not just a mechanical one.
Why does this matter for how to fix bloating? Because if your bloating is primarily a sensation driven by gut nerve sensitivity, dietary changes alone may not resolve it. If it is primarily mechanical — gas, stool, or fluid accumulating — then the approach is different again. Getting this right is the starting point.
The 7 Real Causes of Bloating
Most bloating comes from a short list of well-understood causes. The challenge is that several of these can overlap, and some causes get far more attention online than their actual prevalence warrants. Let’s keep this practical and go through each one honestly.
Gas Production from Fermentation
When you eat carbohydrates — particularly fermentable ones — the bacteria in your large intestine break them down and produce gas as a byproduct. This is completely normal. The issue arises when the volume of gas produced exceeds what the gut can move through comfortably, or when the gut is unusually sensitive to normal gas volumes [4].
Foods high in FODMAPs (fermentable oligosaccharides, disaccharides, monosaccharides, and polyols) are the main drivers here. Beans, lentils, onions, garlic, apples, and certain dairy products are common examples [3]. High-fat meals also slow gastric emptying, which means food sits longer and ferments more [6].
Food Intolerances (Real and Overclaimed)
Lactose intolerance and fructose malabsorption are genuinely common and well-documented causes of bloating. FODMAP sensitivity is real and clinically supported. Non-coeliac gluten sensitivity exists but is far less common than the wellness industry suggests — and in many cases, the culprit is fructans (a FODMAP found in wheat) rather than gluten itself [3].
Here’s the real issue with food intolerance claims: they have become an industry. Many people are told they are intolerant to a long list of foods based on tests that are not clinically validated. We need to separate fact from hype here, and I will come back to this in the section on things that don’t work.
Constipation
This one is consistently underestimated. When the colon is backed up, gas cannot move through efficiently. Bacteria continue fermenting stool contents for extended periods, producing more gas. The result is visible abdominal distension that has nothing to do with what you ate today [1].
Constipation is defined clinically as fewer than three bowel movements per week, but functional constipation — where transit is slow even without meeting that threshold — can cause significant bloating [3]. If you are not clearing your bowel regularly, this is where to start.
Swallowed Air (Aerophagia)
Every time you swallow, a small amount of air goes with it. Fizzy drinks, chewing gum, eating quickly, talking while eating, and drinking through straws all increase the amount of air entering the digestive tract [1]. This air has to go somewhere — usually back up as a belch, or further down as gas.
In real-world terms, aerophagia is probably responsible for more post-meal bloating than most people realise. It’s also one of the simplest things to address.
Low Stomach Acid and Slow Gastric Emptying
Stomach acid plays a role in breaking down protein and triggering the digestive cascade. When acid levels are low — which becomes more common with age — food can sit in the stomach longer than it should, leading to fermentation higher up in the digestive tract [6].
Slow gastric emptying (gastroparesis in its clinical form, but also milder functional slowing) produces a feeling of fullness and bloating that starts early in a meal and lingers for hours. This is more common in people with diabetes and in older adults.
Visceral Hypersensitivity
This is the cause that most generic bloating articles skip entirely. Visceral hypersensitivity means the nerves of the gut are unusually reactive to normal stimuli — pressure, gas, movement — that would not bother someone with a typical pain threshold.
As one gastroenterologist at Houston Methodist has noted, many people who report bloating may not actually have more gas in their intestines than others; their bodies are simply reacting differently to normal amounts of gas [4]. This is a central feature of IBS and explains why some people feel severely bloated even when imaging shows nothing unusual.
Hormonal Fluctuations
For women, this one is significant and often dismissed. In the days before menstruation, estrogen rises and progesterone drops. Estrogen promotes water retention and directly affects gut motility and visceral sensitivity through receptors in the GI tract [5]. The result is bloating that is partly fluid-based and partly neurological — and it follows a predictable monthly pattern.
Perimenopause and menopause bring additional hormonal variability that can make gut symptoms less predictable and harder to manage with standard dietary advice alone.
SIBO: Small Intestinal Bacterial Overgrowth
SIBO occurs when bacteria that normally live in the large intestine colonise the small intestine in excess numbers, fermenting food before it has been properly absorbed [5]. It is a real condition, more common in people who have had abdominal surgery or who have IBS with diarrhoea [1].
That said, SIBO has become significantly overdiagnosed in online 4-week gut healing resetth communities. Breath testing for SIBO has variable accuracy, and many people receive SIBO diagnoses — and expensive treatment protocols — based on tests that are not reliably interpreted. A sensible starting point is to work through the more common causes before pursuing a SIBO workup.

Which Type of Bloater Are You?
Identifying your bloating pattern is more useful than any single dietary change. Here are four honest types — read through them and consider which one fits your experience most closely.
The After-Dinner Bloater
Pattern: You feel fine in the morning, but by evening your abdomen is visibly distended and uncomfortable. It tends to worsen as the day goes on.
What’s likely happening: Cumulative fermentation from meals, portion size, and possibly aerophagia. High-FODMAP foods eaten across the day add up. Evening meals with large portions slow gastric emptying further.
Self-check: Does it happen regardless of what you eat, or only after certain foods? Does it improve when you skip dinner or eat a very light evening meal?
The Chronic Low-Grade Bloater
Pattern: You feel bloated most of the time — not dramatically, but persistently. It’s there when you wake up and doesn’t fully resolve.
What’s likely happening: Constipation or slow gut transit is the most common culprit here. The colon is simply carrying more than it should, and that creates a baseline level of distension [3].
Self-check: How often are you having a complete bowel movement? Is your stool hard or difficult to pass? If yes, start here before looking at diet.
The Specific-Food Bloater
Pattern: You can trace your bloating directly to particular foods — dairy, onions, beans, certain fruits. It’s predictable and reproducible.
What’s likely happening: A genuine food intolerance, most likely FODMAP-related. This is the type where a structured low-FODMAP trial is most likely to give clear answers [3].
Self-check: Can you name the foods that reliably cause it? Does avoiding those foods resolve the bloating within 24-48 hours?
The All-Day Stress Bloater
Pattern: Your bloating tracks your how the gut-brain axis links stress and bloating levels more than your diet. It’s worse during difficult weeks, better on holiday, and present even when you’ve eaten carefully.
What’s likely happening: Visceral hypersensitivity driven by the gut-brain axis. Cortisol affects gut motility and nerve sensitivity. This type of bloating responds poorly to dietary changes alone [5].
Self-check: Does your bloating worsen during stressful periods regardless of what you eat? Does it ease when you’re relaxed, even if your diet hasn’t changed?

What Actually Works: Fixes Matched to Type
The evidence suggests that matching the intervention to the cause is what separates people who get results from those who cycle through every supplement on the shelf. Here’s what the stronger evidence points to for each type.
For the after-dinner bloater:
- Reduce portion size at evening meals
- Identify and reduce your top three FODMAP sources — you don’t need to eliminate everything
- Eat more slowly and without distractions to reduce swallowed air [1]
- Consider a short walk after dinner — light movement supports gastric emptying [6]
- Peppermint oil capsules (enteric-coated) have reasonable evidence for reducing gut spasm and gas discomfort [6]
For the anti-inflammatory eating patterns for chronic gut issues low-grade bloater:
- Address constipation first — this is non-negotiable
- Increase fluid intake and soluble fibre gradually (see the next section on why gradually matters)
- Light daily movement — even a 20-minute walk — meaningfully improves gut transit
- Consider a short trial of a gentle osmotic laxative (such as polyethylene glycol) if dietary changes alone are insufficient — discuss with a pharmacist or doctor
For the specific-food bloater:
- A structured low-FODMAP elimination and reintroduction protocol is the most evidence-supported approach [3]
- Work with a dietitian if possible — the reintroduction phase is where most people go wrong
- Do not stay on a full elimination diet indefinitely — the goal is to identify your specific triggers, not to avoid everything forever
- Lactase enzyme supplements are genuinely useful if lactose is a confirmed trigger
For the all-day stress bloater:
- Dietary changes will have limited impact until the nervous system component is addressed
- Diaphragmatic breathing before meals reduces vagal tone and gut sensitivity
- Eating without screens and in a calm environment is not just good advice — it has a measurable effect on gut motility [1]
- Gut-directed hypnotherapy and cognitive behavioural therapy have clinical evidence behind them for IBS-related bloating [5]
- Low-dose antispasmodics or gut-directed medications may be appropriate — worth discussing with a doctor if self-management isn’t working
The Fiber Paradox
how to ramp up fiber without making bloating worse is both a cause and a cure for bloating, depending on context. This is where a lot of well-meaning advice goes wrong.
Too little fibre leads to constipation, which leads to the chronic gut issues and the leaky gut evidence low-grade bloating described above. But too much fibre, added too quickly, dramatically increases fermentation in the colon and can make bloating significantly worse — particularly insoluble fibre from bran and high-fibre cereals [6].
The type of fibre matters too. Soluble fibre (oats, psyllium, cooked vegetables) is generally better tolerated than insoluble fibre (wheat bran, raw vegetables, whole grains) for people who are already bloating. And the pace of introduction matters as much as the amount — the gut’s bacterial population needs time to adapt.
The practical rule: if you are increasing fibre to address constipation-related bloating, do it slowly over two to three weeks, increase water intake alongside it, and favour soluble sources first. For more detail on [the right way to increase fibre without making bloating worse], see [LINK: Fiber article]. For a longer-term approach to gut health, [a structured 4-week gut reset] is covered in [LINK: Heal Your Gut article].
Things That Usually Don’t Work (But Get Recommended Anyway)
This is where hype gets in the way of actual progress. Let’s call it what it is.
Activated charcoal capsules: Charcoal does bind gas in the gut, but it also binds nutrients, medications, and beneficial compounds. The evidence for meaningful bloating relief is weak, and the risk of interfering with medication absorption is real. I would be careful with that one, particularly if you take any regular medications [6].
IgG food sensitivity tests: These tests measure IgG antibodies to various foods, but IgG antibody presence indicates exposure, not intolerance. That is a strong claim and needs strong proof — and the clinical evidence simply does not support IgG testing as a valid diagnostic tool for food intolerance. Major gastroenterology bodies do not recommend them [3]. They are expensive, they generate long lists of foods to avoid, and they frequently lead people to unnecessary restriction.
“Detox” teas: Most products marketed as detox or cleansing teas contain senna or other stimulant laxatives. They may produce a temporary feeling of flatness by clearing the bowel, but they do not address the underlying cause of bloating. Regular use of stimulant laxatives can impair normal bowel function over time.
Apple cider vinegar shots: The evidence here is genuinely weak. The proposed mechanism — that ACV increases stomach acid — is plausible in theory but not well-supported in clinical data. In plain bland-food approach that gives your gut a break English: there is no reliable evidence that ACV shots reduce bloating in any meaningful or consistent way.
Long-term elimination diets with no reintroduction plan: Removing foods indefinitely without a structured reintroduction phase is not a treatment — it’s avoidance. It narrows the diet unnecessarily, risks nutritional gaps, and does not help identify which foods are actually problematic. The low-FODMAP diet is designed as a short-term diagnostic tool, not a permanent eating pattern.
When Bloating Is Actually a Red Flag
Most bloating is functional — uncomfortable but not dangerous. However, there are specific combinations of symptoms that warrant prompt medical attention, not a trip to the supplement aisle.
See a doctor if bloating is accompanied by:
- Unintentional weight loss
- Blood in the stool or rectal bleeding
- Severe or worsening abdominal pain
- Persistent vomiting
- A significant change in bowel habits lasting more than two weeks
- Bloating that does not vary — it is present all the time and does not improve
In women specifically, persistent bloating that does not respond to dietary changes and is accompanied by pelvic discomfort or changes in urinary frequency should be evaluated. Ovarian cancer can present with bloating as an early symptom, and it is frequently misattributed to digestive issues for months before investigation [5].
The message here is not to panic — the vast majority of bloating is benign. But don’t spend six months trialling supplements when a GP appointment could rule out something that needs actual treatment. For guidance on when digestive symptoms warrant investigation, see [LINK: Common Health Symptoms Decoded: When to Worry and When to Wait].
A 7-Day Bloating Reset
This is a practical reset, not a diet. The goal is to reduce the most common bloating triggers, add specific supports, and gather information about your own pattern. Most people should not stay on a modified eating plan long-term — the point is to identify what’s driving the problem.
Days 1-2: Remove the easy offenders
- Cut fizzy drinks and sparkling water
- Stop chewing gum
- Avoid artificial sweeteners (sorbitol, xylitol, mannitol — common in sugar-free products)
- Reduce portion sizes at your largest meal
Days 3-4: Add specific supports
- Drink ginger tea (fresh ginger steeped in hot water) before or after meals — ginger has reasonable evidence for supporting gastric motility [6]
- Try enteric-coated peppermint oil capsules if gut spasm is part of your pattern
- Eat slowly, seated, without screens
- Add a 15-20 minute walk after your main meal
Days 5-6: Low-FODMAP trial if symptoms persist
- If bloating is still significant, reduce your top FODMAP sources: onions, garlic, apples, pears, beans, and milk-based products
- This is not about eliminating everything — target the highest-FODMAP items in your current diet
- Keep a simple food and symptom log
Day 7: Reassess
- Which changes made the most difference?
- Is your pattern after-dinner, chronic, food-specific, or stress-driven?
- Use this information to decide whether a structured low-FODMAP protocol, a constipation-focused approach, or a gut-brain intervention is the right next step
The Gut-Brain Piece Most Articles Ignore
Stress-driven bloating is real, and it is not in your head — it is in your nervous system. The gut contains more nerve cells than the spinal cord, and it communicates constantly with the brain via the vagus nerve. When stress activates the sympathetic nervous system, gut motility slows, visceral sensitivity increases, and the perception of pain and pressure rises [5].
Cortisol — the primary stress hormone — directly affects gut function. This is why people with high-stress lives often experience bloating that tracks their mental state more closely than their diet. It is also why IBS is classified as a disorder of gut-brain interaction, not simply a digestive disease [7].
The practical interventions here are simple and underused. Diaphragmatic breathing for five minutes before a meal activates the parasympathetic nervous system and genuinely improves gut function. Eating without screens reduces the stress load on the digestive process. Slowing down is not just a polite suggestion — it changes the physiological environment in which digestion happens. These are not soft recommendations. The evidence supports them [1].
Frequently Asked Questions
1. Why am I bloated even when I haven’t eaten?
Bloating without recent food intake is most commonly caused by constipation or slow gut transit — the colon is carrying accumulated stool and gas regardless of what you’ve eaten today [3]. It can also reflect visceral hypersensitivity, where the gut is reacting to normal internal pressure. Hormonal fluctuations, particularly in the days before menstruation, can also cause bloating independent of food intake [5].
2. Does drinking water help bloating?
It depends on the cause. Adequate hydration supports gut motility and helps prevent constipation, which is one of the most common causes of bloating [1]. However, drinking large amounts of water quickly, or drinking carbonated water, can temporarily worsen bloating by adding volume or gas to the digestive tract. Sipping water steadily through the day is more useful than drinking large amounts at once.
3. What’s the fastest way to reduce bloating?
For immediate relief, the most effective options are: a short walk to encourage gut motility, enteric-coated natural ways to soothe your stomach oil capsules for gas-related discomfort, and avoiding further gas-producing foods or carbonated drinks for the next few hours [6]. If constipation is the driver, a gentle osmotic laxative works faster than dietary changes. There is no single fastest fix because the answer depends on the cause.
4. Is bloating the same as water retention?
No. Bloating is primarily caused by gas or gut contents in the digestive tract. Water retention (oedema) is fluid accumulating in body tissues, often in the hands, feet, and face. They can occur simultaneously — particularly around menstruation, when both gut bloating and fluid retention are driven by hormonal changes [5] — but they have different causes and different solutions.
5. Can probiotics cause bloating?
Yes, and this is more common than most probiotic marketing acknowledges. When you introduce new bacterial strains to the gut, there is often a period of adjustment during which gas production temporarily increases. This usually settles within one to two weeks. However, in people with SIBO, probiotics can significantly worsen symptoms [1]. If bloating increases substantially after starting a probiotic and does not improve within two weeks, stop and reassess.
6. How long is too long to be bloated?
Bloating that lasts more than a few days without a clear dietary explanation, or that is present consistently for more than two weeks, warrants attention. Bloating that is accompanied by other symptoms — pain, weight loss, blood in stool, or changes in bowel habits — should be evaluated by a doctor promptly, not managed with home remedies [5]. Occasional bloating is normal. Persistent, unchanging bloating is not something to manage indefinitely without investigation.
Key Takeaways
- Bloating and distension are not the same thing. The sensation of bloating is partly neurological, which is why dietary changes alone don’t always work.
- There are seven distinct causes of bloating, ranging from fermentation and constipation to hormonal changes and visceral hypersensitivity. Identifying your cause is more useful than any single remedy.
- Your bloating type determines your fix. After-dinner, chronic, food-specific, and stress-driven bloating each respond to different interventions.
- Constipation is the most consistently overlooked cause of persistent, low-grade bloating. Address it before trying elimination diets.
- Several popular remedies — activated charcoal, IgG sensitivity tests, detox teas, apple cider vinegar — have weak or no clinical evidence and some carry real risks.
- The gut-brain connection is not a soft concept. Stress, cortisol, and vagal tone directly affect gut function and bloating. Behavioural interventions have genuine clinical support.
- Persistent bloating with weight loss, blood in stool, or pain lasting more than two weeks is a medical matter, not a dietary one. See a doctor.
Conclusion
Bloating is not one problem. It is several — each with a different mechanism, a different pattern, and a different fix. The reason so many people cycle through advice without getting results is that they are applying generic solutions to a specific problem they haven’t yet identified.
The basics still do the heavy lifting here: address constipation, reduce your top FODMAP sources if food is the trigger, slow down at meals, and take the gut-brain connection seriously. If those don’t move the needle, a structured low-FODMAP protocol with proper reintroduction — ideally guided by a dietitian — is the most evidence-supported next step.
What matters most is this: you don’t need a more expensive supplement or a longer list of foods to avoid. You need a clearer picture of what’s actually driving your bloating. Start there, match the fix to the type, and keep it simple and consistent.
Most bloating isn’t mysterious. It’s just been badly explained.

References
- [Video] Dr. YouTube. https://www.youtube.com/watch?v=jt5hHb6kzYM